Women’s health behaviour & cervical screening
Four of the most widely used SCMs, namely the Protection Motivation Theory (PMT, Rogers 1975), the Health Belief Model (HBM, Rosenstock, 1974), the Transtheoretical Model (TTM, DiClemente, 1993) and the Theory of Reasoned Action (TRA, Fishbein & Ajzen, 1975)/Theory of Planned Behaviour (TPB, Ajzen & Madden, 1986) have ben employed in the area of preventative health, such as cervical screening (Marteau, 1989). These models and their applications will be described in the following sections.
The basis for all SCMs is the assumption that an individual’s behaviour is a deliberative decision-making process, determined by a dynamic interaction of all the individual’s subjective thoughts and the available stimuli derived from the environment (Conner & Norman, 2005). In other words, an individual’s decision to perform a specific health behaviour is a result of a deliberate subjective cost-benefit evaluation, whereby different courses of action, such as attending for cancer screening are considered. It can be argued that such an approach is concerned with making a trade-off between several options with different probabilities and utilities (i.e., the subjective evaluation of that outcome (Baron & Baron, 1994)). This approach is rooted in the expectancy-value theory (Peak, 1955) and the subjective expected utility theory (SEU, Edwards, 1954), which postulates that individuals aim to maximize utility, such as health, and therefore choose the behaviour which is most likely to achieve the highest expected utility after having evaluated the benefits and costs of a specific health problem, such as breast or cervical cancer. The PMT, HBM and the TPB all have these underlying assumptions.
In the following section, the one stage model (TTM) of behaviour change will be discussed alongside three continuum models (PMT, HBM and TRA/TPB). For clarification, the difference between stage and continuum models of behaviour change is in the nature of the relationship between beliefs and behaviour. That is to say, that stage models, such as the TTM, consider individuals as being at distinct and qualitatively different stages of the process of behavioural change (Sutton, 2002). Continuum models, on the other hand, place individuals along a continuum of expectancy.
Stage Models of Behavioural Change
Transtheoretical Model (TTM)
The Transtheoretical Model of behaviour change was originally introduced to explain the history of remission and relapse in addictive disorders (DiClemente, 1993). In essence, the model provides an understanding of how people change their behaviour. The underlying assumption is that people move through changes and that each stage is profoundly different from the last. The model includes five sequential stages, ten processes (experiental and behavioural) – which individuals mostly use to facilitate change, decisional balance (pros and cons) and self-efficacy (the individual’s confidence and temptations that they can make changes).
Stages of Change
The model consists of five stages that are outlined below (adapted from Prochaska, Redding & Evers, 2002):
- Pre-contemplation: The individual does not exhibit and has no intention of changing or adopting a new behaviour within the next six months;
- Contemplation: The individual is considering adopting the behaviour (within the next six months), but has not dedicated any effort towards enacting it or preparing to enact it;
- Preparation: The individual has started to gather information on the behaviour, with a view towards enacting it (within the next 30 days).
The above three stages are also described as pre-action stages, whereas the following two stages are the post-action stages (Sutton, 2005):
- Action: The individual has begun to enact the behaviour regularly, but has not continued doing so over a long period (for less than six months);
- Maintenance: The individual has been regularly enacted the behaviour for more than six months.
Whilst the model proposes that individuals are moving through these distinct stages, at the same time it acknowledges that some may relapse from ‘action’ or ‘maintenance’ to an earlier stage. The actual processes of change are the covert and overt activities that help individuals in progressing through the stages of change. There are five experiential and five behavioural processes that are listed below.
Experiental Processes:
- Consciousness raising: Finding facts and information that support the change in behaviour;
- Dramatic relief: Experiencing the negative emotions that accompany the unhealthy behaviour;
- Self re-evaluation: Recognizing the change as a significant part of one’s identity by contrasting the image before and after the change;
- Environmental re-evaluation: Recognition of how the individual’s behaviour affects those around them;
- Self-liberation: Believing that one can change and make a firm commitment to change.
Behavioural Processes:
- Helping relationships: Seeking social support for making the change in behaviour;
- Counter-conditioning: Substituting healthier alternatives or safer options for the problem behaviour;
- Reinforcement management: Reinforcing positive behaviour and reducing rewards for the negative/unhealthy behaviour;
- Stimulus control: Removing reminders of the negative/unhealthy behaviour and adding cues and reminders for the desired behaviour;
- Social liberation: Realizing that the social norms are changing in the direction of supporting the change in behaviour.
The above processes are linked to the stage of change, suggesting that as one progresses across the stage of change, there is a shift from these different influences.
Application and Effectiveness
The TTM has been utilized in a number of health-related settings such as smoking cessation (Etter & Sutton, 2002; Sutton, 2000), exercise (Cox, Gorley, Puddey, Burke & Beilin, 2003), condom use (Harlow, Prochaska, Redding, Rossi, Velicer, Snow, Schnell, Galavotti, Reilly, Rhodes, 1999), substance use (Sutton, 2001) and cervical screening (Eiser & Cole, 2002).
In order to explore the model’s effectiveness in terms of correctly predicting discontinuity patterns, Rosen (2000) carried out a meta-analysis examining 34 studies. For clarification, exploring discontinuity patterns means examining whether certain variables are increased between certain stages such as between Stage I and Stage II, whilst not showing any difference between other stages, e.g., Stage II and Stage III. One of the findings was that in 85% of all studies investigated, behavioural processes peaked during action or maintenance stage. These are the stages, according to Prochaska et al. (2002) in which behavioural processes are predicted to peak, whereas the experiental processes are expected to decline. In terms of the increase of experiental processes, Rosen (2000) reported that in 41% of all studies investigated, these processes peaked in the contemplation or preparation stage as proposed by Prochaska et al. (2002). It was, however, also noted that there was inconsistency in the use of these different change processes at different, unexpected stages across a number of health behaviours.
Limitation of TTM
As outlined above, the TTM makes suggestions for the duration of time that the individual may stay in a stage before progressing to the next, for example, moving from the contemplation (enacting within the next six months) to preparation stage (thinking of changing within the next 30 days). Kraft, Sutton and McCreath-Reynolds (1999) argue that there is little empirical evidence that these stages are qualitatively different.
Marks, Murray, Evans and Willig (2000) reported that the model inadequately addresses the social aspect in which many health behaviours, such as drinking alcohol, actually occur.
Further, it has been commented that this model is: “…neither a theory nor a model, but a tautological description of what must logically occur” (Roberts et al., 2001, p. 81).
Continuum Models of Behaviour Change
In the following section, three of the most widely employed models (PMT, HBM, TRA/TPB) will be outlined and discussed.
Protection Motivation Theory
The Protection Motivation Theory (PMT, Rogers 1975) was originally proposed to provide clarity to the understanding of fear appeals and it was extended eight years later (Rogers, 1983) to allow a more general application. Thereby more prominence was given to the underlying cognitive processes which may mediate behavioural changes.
Essentially, Roger’s model consists of four key constructs, which predict people’s health behaviour:
- Perceived threat
- Perceived vulnerability
- Response efficacy
- Self-efficacy.
Together these four beliefs comprise two appraisal pathways (threat and coping), which determine people’s subsequent protection motivation.
Figure 1 below is a graphical representation of the model (adapted from Conner & Marks, 2005).
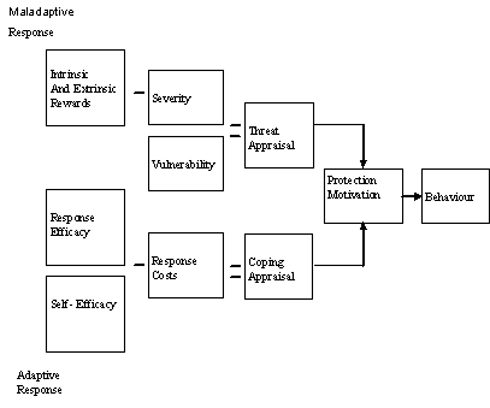
Figure 1: The Protection Motivation Theory
It can be seen from the graphic representation above that the theory postulates that people’s intention to protect themselves from a health threat, for instance breast cancer, is the result of the evaluation of their threat and coping appraisal. More precisely, in completing their threat appraisal people estimate the seriousness (or severity) of the disease as well as their own vulnerability to this disease (e.g., the likelihood of having breast cancer).
Their coping appraisal, on the other hand, consists of their response efficacy as well as self-efficacy. The former refers to people’s expectancy that performing a recommended action would remove the threat, whilst self-efficacy is people’s belief in their own ability to execute the recommended action or behaviour and therefore to avert the health threat.
Evaluating the two appraisal pathways subsequently determines people’s decisions and outcomes, leading to either an adaptive response, for example, women accept their breast screening invitation or a maladaptive response/behaviour whereby women decide to reject their screening invitation.
Application and Effectiveness
The PMT has been used for a variety of areas, such as sun protective behaviour (Azzarello, Dessureault & Jacobsen, 2006), smoking cessation (Maddux & Rogers, 1983), condom use (Tanner, Hunt & Eppright, 1991), sexual health (Blanton & Gerrad, 1997), breast screening (McCaul, Reid, Rathge & Martinson, 1996), colorectal screening (Vernon, Myers, Tilley & Li, 2001) and prostate cancer screening (Vadaparampil, Jacobsen, Kash, Watson, Saloup & Pow-Sang, 2004).
In terms of the model’s effectiveness, meta-analyses carried out by Floyd, Prentice-Dunn and Rogers (2000) and Milne, Sheeran and Orbell (2000) showed that, overall, the model’s variables were able to significantly predict intention and behaviours, but they were less able to predict future behaviour. Both meta-analyses indicated that threat appraisal had small effect sizes, whereas coping appraisals were found to be of medium effect size (Norman, Boer and Seydel, 2005). It was noted, however, that the model was weaker in its ability to predict future behaviour.
Limitation of PMT
One limitation of this model is that it puts the primary focus on people’s intention and to a lesser extent on their subsequent behaviour (Prentice-Dunn & Rogers, 1986). A study by Orbell and Sheeran (1998) concerning breast self-examination also showed that the model was unable to discriminate between women who had the intention of examining their breasts from those who had no intention. The model was also unable to account for women’s future behaviour.
Besides, it has been acknowledged by a number of researchers, such as Vadaparampil et al. (2004) that, whilst the PMT has been employed within a variety of health domains, it is less utilized within the cancer screening setting and in particular within the context of cervical screening.
References
Ajzen, I and Madden, T (1986) Prediction of goal-directed behavior: attitudes, intentions, and perceived behavioral control. J Exp Soc Psychol, 22, 453-474.
Azzarello, L, Dessureault, S and Jacobsen, P (2006) Sun-Protective Behavior among Individuals with a Family History of Melanoma. Cancer Epidemiol Biomarkers Prev, 15, 142-145.
Baron, J and Baron, J (1994) Thinking and Deciding, University Press, New York: Cambridge.
Blanton, H and Gerrad, M (1997) Effect of Sexual Motivation on Men’s Risk Perception for Sexually Transmitted Disease: There Must Be 50 Ways to Justify a Lover. Health Psychology, 16, 374-379.
Conner, M and Norman, P (eds) (2005) Predicting Health Behaviour (2nd edn) Open University Press, Buckingham.
Cox, K, Gorely, T, Puddey, D, Burke, V and Beilin, L (2003) Exercise behaviour change in 40 to 65-year-old women: the SWEAT study (Sedentary Women Exercise Adherence Trail). British Journal of Health Psychology, 8, 477-95.
Edwards, W (1954) The Theory of Decision Making. Psychol. Bull. 51, 380-417.
Eiser, R and Cole, N (2002) Participation in Cervical Screening as a Function of Perceived Risk, Barriers and Need for Cognitive Closure. Journal of Health Psychology, 7, 99-105.
Etter, J F and Sutton, S (2002) Assessing ‘stage of change’ in current and former smokers. Addiction, 97, 1171-82.
Fishbein, M and Ajzen, I (1975) Belief, attitude, intention and behavior: An introduction to theory and research, Addison-Wesley, Reading.
Floyd, D, Prentice-Dunn, S. and Rogers, R (2000) A meta-analysis of research on protection motivation theory. Journal of Applied Social Psychology, 30, 407-429.
Harlow, L, Prochaska, J, Redding, C, Rossi, J, Velicer, W, Snow, M, Schnell, D, Galavotti, C, O’Reilly, K and Rhodes, F (1999) Stages of condom use in a high HIV-risk sample. Psychology and Health, 14, 143-157.
Kraft, P, Sutton, S and McCreath-Reynolds, H (1999) The Transtheoretical model of behaviour change: are the stages qualitatively different? Psychology and Health, 14, 433-50.
Maddux, J and Rogers, R.W (1983) Protection motivation theory and self-efficacy: A revised theory of fear appeals and attitude change. Journal of Experimental Social Psychology, 19, 469-479.
Marks, D, Murray, M, Evans, B and Willig, C (2000) Health Psychology: Theory, Research and Practice. Sage, London.
Marteau, T (1989) Psychological costs of screening. BMJ, 299, 527.
McCaul, K, Reid, P, Rathge, R and Martinson, B (1996) Does Concern About Breast Cancer Inhibit or Promote Breast Cancer Screening? Basic and Applied Social Psychology, 18, 183-194.
Milne, S, Sheeran, P and Orbell, S (2000). Prediction and intervention in health-related behaviour: A meta-analytic review of protection motivation theory. Journal of Applied Social Psychology, 30, 106-143.
Norman, P, Boer, H and Seydel, E (2005) Protection Motivation Theory. In Conner, M and Norman, P (eds) (2005) Predicting Health Behaviour: Research and Practice with Social Cognition Models, Open University Press, Maidenhead.
Orbell, S and Sheeran, P (1998) ‘Inclined abstainers’: A problem for predicting health-related behaviour. British Journal of Social Psychology, 37, 151-165.
Peak, H (1955) Attitude and motivation. In Conner, M and Norman, P (eds). (2005) Predicting Health Behaviour (2nd edn), Open University Press, Buckingham.
Prentice-Dunn, S and Rogers, R (1986) Protection Motivation Theory and preventive health: beyond the health belief model. Health Education Research, 1, 153-161.
Proachaska, J, Redding, C and Evers, K (2002) The Transtheoretical model and stage of change. In Glanz, K, Rimer, B K and Lewis, F M (2002) Health Behavior and Health Education: Theory, Research, and Practice (3rd edn), Jossey-Bass, San Francisco.
Roberts, R, Towell, T and Golding, J (2001) Foundations of Health Psychology, Great Palgrave, Britain.
Rogers, R (1983) in Orbell,S and Sheeran,P. (1998) ‘Inclined abstainers’: A problem for predicting health-related behaviour. British Journal of Social Psychology, 37, 151-165.
Rogers, G (1975) A protection motivation theory of fear appeals and attitude change. J Psychol, 91, 93-114.
Rosen, C (2000) Is the sequencing of change process by stage consistent across health problems? A meta-analysis. Health Psychology, 19, 593-604.
Rosenstock, I M (1974) The health belief model and preventive health behavior. In Bandura, A (1998) Health Promotion From The Perspective of Social Cognitive Theory. Psychology and Health, 13, 623-649.
Sutton, S (2005) Stage Theories of Health Behaviour. In Conner, M and Norman, P (eds) (2005) Predicting Health Behaviour (2nd edn), Open University Press, Buckingham.
Sutton, S (2000). A critical review of the transtheoretical model applied to smoking cessation. In Norman, P, Abraham, C, and Conner, M (2000) Understanding and Changing Health Behaviour: from Health Beliefs to Self-regulation. Harwood Academic Press, Reading.
Sutton, S (2001) Back to the drawing board? A review of applications of the transtheoretical model to substance use. Addiction, 96, 175-186.
Tanner, J F, Hunt, J and Eppright, D R (1991) The protection motivation model: a normative model of fear appeals. Journal of Marketing, 55, 36-45.
Vadaparampil, S, Jacobsen, P, Kash, K, Watson, I, Saloup, R and Pow-Sang, J (2004) Factors Predicting Prostate Specific Antigen Testing among First-Degree Relatives of Prostate Cancer Patients. Cancer Epidemiol Biomarkers Prev, 13, 753-758.
Vernon, S, Myers, R, Tilley, B and Li, S (2001) Factors Associated with Perceived Risk in Automotive Employees at Increased Risk of Colorectal Cancer. Cancer Epidemiology Biomarkers & Prevention, 10, 35-43.