Essay on Measles and MMR Vaccine
Number of words: 2737
The MMR vaccine is a vaccine used universally which protects individuals against (German) measles, mumps and rubella. Although each viral disease had its own vaccine, the combined MMR was developed by microbiologist Maurice Hilleman and licensed in 1971(1). This version is believed to induce a faster and less painful immunity (1). Similar to the tuberculosis (BCG) and yellow fever vaccine, this vaccine type is a live and attenuated vaccine (consisting of live weakened virus), therefore it has its infectious components altered to become less harmless. After administration, immune cells (lymphocytes) produce antibodies and specific B-cells (part of the acquired immune system) against the antigen are formed (2).
Figure 1- This diagram shows the mechanism of vaccinations and the immune response against the virus (3).
Furthermore, unlike other countries, immunisation is not compulsory in the United Kingdom, but it is recommended that children are given two doses of the vaccine. The first at twelve months and the second (booster dose) between three to five years (1). Aside from its more obvious benefits of protecting against a rash, cough, fever, muscle pain and arthritis that accompanies the three diseases. MMR can prevent and control the more serious and often fatal complications such as pneumonia, seizures, brain damages (encephalitis) and miscarriages (3). The main aim of this prophylactic vaccine is not only to prevent an infection after vaccination of the given individual, but it also prevents the spread of the virus in a population (3). If a sufficiently high proportion of individuals are immunised, there will be a resistant to the spread of the contagious diseases (3).
Despite the fact that there is hard scientific evidence to support the administration of the MMR vaccination, for example, the decline of the killer disease measles which supresses the whole immune response, making those affected susceptible to more infections (4). Many parents and medical professionals argue that measles is an inevitable stage of a child’s development and discuss the necessity of immunization (5). In addition to the side effects, for example: temperature; rash and loss of appetite, many believe that the vaccine can increase chances of disease such as measles or even worse contribute towards autism and bowel disease (6). Factors such as unfamiliarity with the vaccine also contribute to the decline in the number of babies and children getting vaccinated (6).
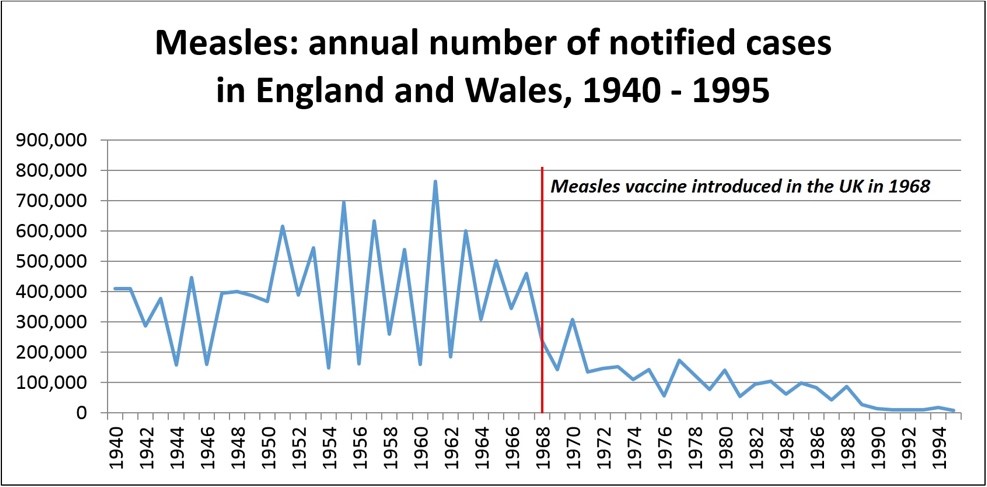
Figure 2- This graph reports the number of measle cases between the years 1940-1995. There appears to be a dramatic decline after the introduction of its vaccine in 1968 (4).
Measles virus is highly contagious and remains a leading cause for infant mortality. Although this disease is restricted to humans only, its eradication still remains difficult and there are often outbreaks of the virus (7). Accurate numbers of occurrence are difficult to obtain due to many cases not being reported, however, prior to the introduction of the vaccine it was estimated that measles caused over two million deaths annually (7). Although one would assume that measles outbreaks take place in developing countries or those with low vaccination and poor sanitation (i.e. The Democratic Republic of the Congo where the numbers of infected individuals is rising), recent data suggest that they exist in developed and resource-rich areas (7). In the UK, there has been an eruption in the cases of measles between January and October of 2018 (913 confirmed cases). It is believed that these incidents were due to individuals not taking their MMR vaccination when they were younger and also due to unvaccinated and infected travellers (this highlights the fact that migration is also a major contributor) (7) (8).
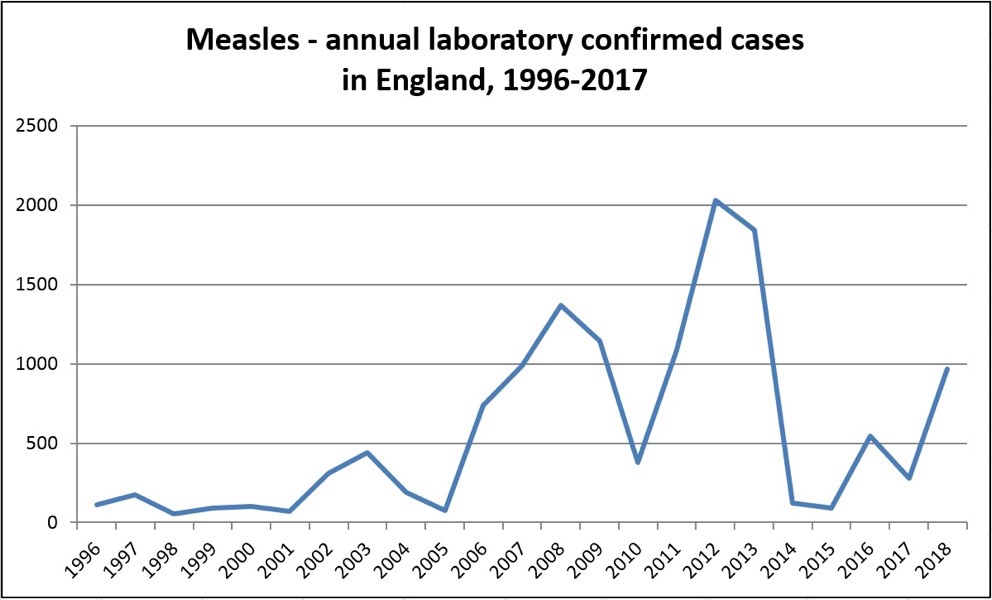
Figure 3- This graph shows the number of measles cases in England between 1996-2017, it can be seen that the highest number was between 2012-2013 (4). There appears to be a steep decline after that and followed by a rise in the numbers in 2018 (4).
In addition, measles is a very communicable disease and is transmitted from person to person via respiratory droplets (coughing and sneezing). Any droplet containing the virus can be suspended in the air or surface for up to two hours. The maximally contagious phase of the infection is during the prodromal phase which is characterised by intense coughing (9). As the mode of transmission is airborne, it means it can be spread very fast and some studies even suggest that it spreads even faster than other viruses such as Ebola and HIV (10). As a result of its fast advancement, epidemics can quickly develop into pandemics, consequently it needs to be controlled.
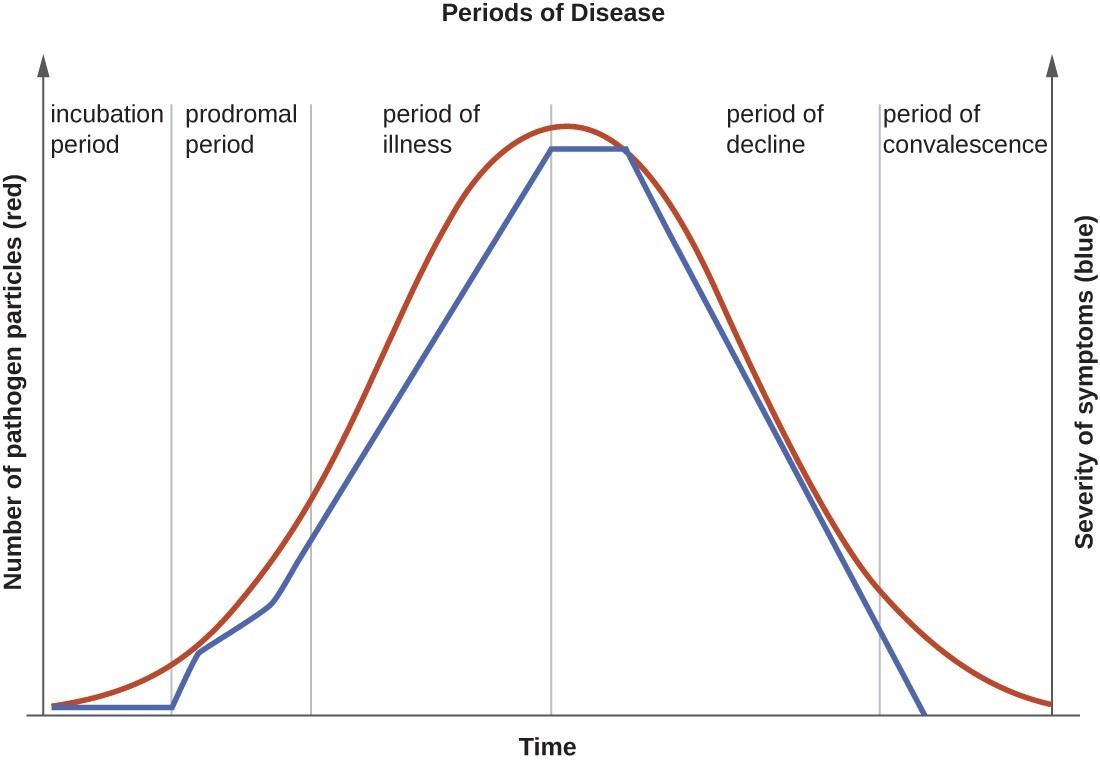
Figure 4- This graph shows the five stages of the progression of an infectious disease (11). The incubation period for measles is usually between 10-14 days and initial symptoms generally arise in the prodromal period which generally consist of malaise, conjunctivitis and coryza (11).
Figure 5- Diagram showing the number of reported cases of measles world-wide from April to September (2015) (12). This data suggests that among all of the countries, measles is concentrated within three of the largest populated places: China; India and Nigeria. This is a major threat as it suggests that not only are many people infected but the disease can also expand very rapidly.
The constituent viral strains of the Mumps, measles and rubella vaccine require animal or human cells as a host for production and thus were formed by breeding them in both animal and human cells (1). With regards to the mumps and measles, they were grown in embryonated hens’ eggs and chick embryo cultures (1). And consequently, were more adapted for hens’ egg rather than human cells (these strains were referred to as the attenuated strains or sometimes even neuroattenuated as they have less virulence in human neurons compared to the wild strains) (1). Furthermore, Meruvax, which is the rubella component was developed in 1967 using human embryonic lung cell line (1). The production of the MMR vaccine was revolutionary in eradicating deadly diseases, since its development there has been numerous documents supporting its use and its benefits in preventing illness, disability and death (1).
In addition to the adverse reactions that may occur due to the administration of the vaccine (malaise and fever). Other factors such as unfamiliarity with the ingredients within the vaccine also contribute to the decline in the number of babies and children getting vaccinated (6). Many parents are also concerned with anaphylaxis and allergic reactions towards the components in the vaccine (1). Acute disseminated encephalomyelitis and transverse myelitis are both examples of rare complications that can arise (1).
In 1998, a gastroenterologist Andrew Wakefield, published a fraudulent paper which linked the development of bowel symptoms and autism after administration of the MMR vaccine (1). Wakefield’s paper involving the twelve children was found to be dishonest and his anti-vax efforts were dismissed (his sample was too small) (1). His deliberate falsification cost Wakefield his medical licence and he was revoked off the UK medical register (1). Furthermore, speculations about the MMR vaccine grew due to the use of thimerosal mercury. Thimerosal is a mercury-containing compound that prevents the growth of bacteria and fungus and is widely used in flu vaccines (as a preservative) to prevent contamination (13). Although there is no significant evidence of harm caused by thimerosal vaccines, in 1999, the U.S. Public Health Service recommended that they should be removed as a precaution (14). In spite of the fact that MMR does not contain thimerosal, fear due to the lack of education around the topic has resulted many anti-vax movements (14). Numerous studies have stated that thimerosal is not a causative agent towards the development of autism and even when this ingredient was removed the rates of autism continued to rise, therefore completely disregarding this theory (14).
Moreover, it is important to take into consideration the two different types of mercury which are completely different materials (13). Firstly, methylmercury is formed in the environment when mercury metal is present and usually present in some types of fish. This can cause damage to the nervous system (in high amounts) and thus, there have been guidelines placed in the United States to reduce levels of exposure (13). On the other hand, thimerosal contains ethylmercury, this type causes less harm as it is broken down by the body (into ethylmercury and thiosalicylate) in a different manner and clears out of the blood more rapidly (less likely to cause harm) (14).
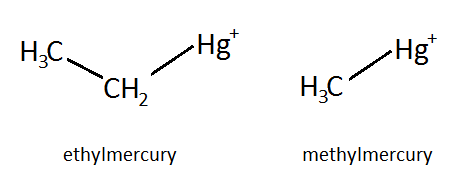
Figure 6- Structural differences between ethyl and methylmercury (15).
In regard to Dr Wakefield’s paper, since its release, overwhelming data and evidence have been released which state that there is no link between MMR vaccine and autism. For example, in Denmark, Madsen and her colleagues compared the occurrence of autism in children who had had the MMR vaccinations and those who did not and discovered that there is no difference (16). In the UK, research conducted by Taylor (London) also revealed no specific link between the two (16). Although no research is without its flaws, it is unlikely that all of them failed to recognise that there is in fact a link between MMR and autism (16). An expert group in Scotland comprising of medical specialists, parents and also representatives of autism support group deduced that the current scientific evidence does not show or support a link between the vaccine and the developmental disorder (17).
To ensure that the spread of these deadly diseases is prevented, it is vital for healthcare professionals to be knowledgeable and confident about the vaccinations. This is because while parents make the final decision on whether or not to immunize their child, their decision is largely influenced by health professionals (18). This will mean that the public will not receive misinformation and therefore decide to do what is more beneficial for their children (which is immunisation). Numerous studies involving communication, reveal that there is a lack of knowledge about the vaccinations and that they are not always due to lack of education but also due to cultural, religious (use of gelatine stabilizer) and personal beliefs (18). Although lack of knowledge may be of the easier challenges to face, false perceptions (in particular the benefit-risk ratio) and social beliefs often require more effort (18). As social media has a strong influence people’s attitudes, in order to stop vaccination rates dropping, it is vital to create a step-by-step approach and create a platform to disseminate the correct information nationally (18). With reference to this particular case, the mother needs to understand that her aunt’s advice is not from a medical professional and is a matter of opinion (from old false scientific research), thus basing her decision off of that would be extremely wrong of her (18). She cannot ask a science student advice as he/she is not qualified to make a decision. By speaking to a paediatrician or pharmacist she will have a greater knowledge of the contents within (mercury) and also the benefits and risks (18). Another point to consider is that mother herself is likely to have been vaccinated, as if she did not her daughter may have been born with congenital defects (something that can happen to her grandchild given that she doesn’t vaccinate her daughter) and the mother herself is also not autistic , therefore completely disproving her aunts claims of the side effects of the vaccine.
Overcoming the barriers to MMR vaccination is fundamental to the eradication of the three diseases and thus progression of the medical and scientific field. Furthermore, it would be beneficial for regulatory bodies to establish a set of laws which increases the uptake of MMR vaccine, for example, children must provide evidence of both doses of MMR vaccinations prior to starting school. This not only ensures that the spread is controlled but also emphasises on the importance of taking the second dose as well (which is needed for complete immunity).
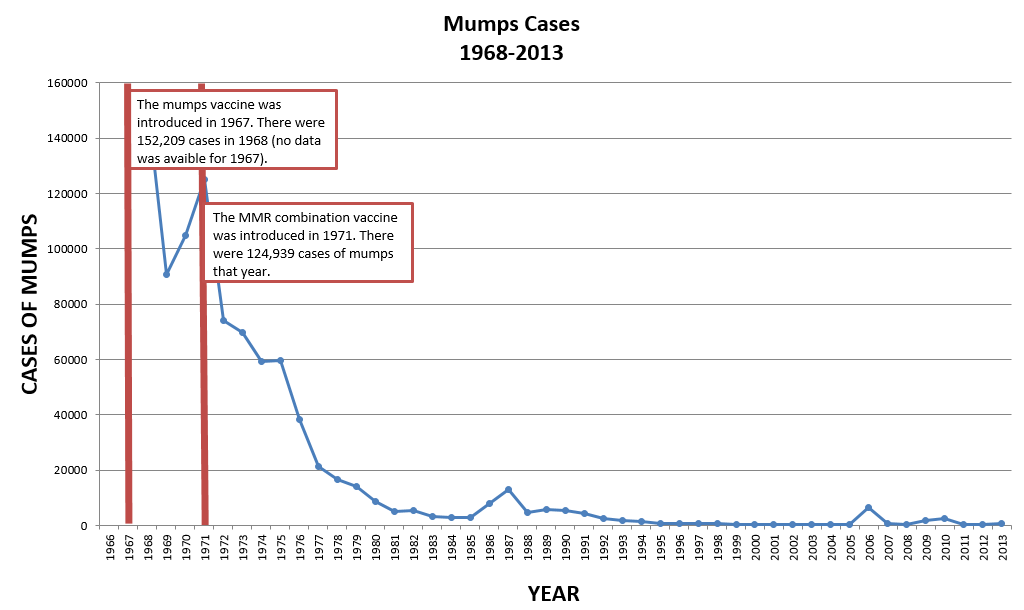
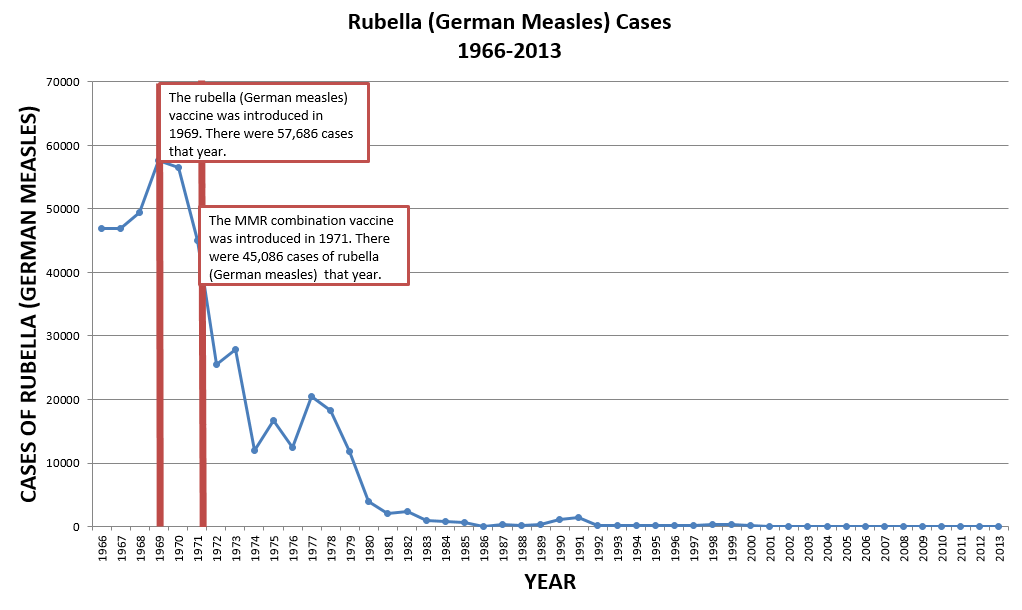
Figure 7 and 8- Graphical illustration of the number of cases of both mumps and rubella prior to and after MMR vaccination. Both show a dramatic decline (19)
In conclusion, the benefits of vaccination against most diseases (in this case MMR) clearly outweigh the negatives. This is not only shown by the decline of the cases but also eradication of some. The World Health Organization (WHO), has extended its target date from 2015 to 2020 for the eradication of measles in all European countries (except Germany) (20). In order to reach this milestone, like America, Europe needs to achieve a >95% vaccination rate (20). Although, one possible solution to the eradication is to make the vaccinations compulsory, the reactions and effects to this action are unpredictable (20). The authorities may face greater resistance and their motives may be put under question. Understanding the benefits of the MMR vaccination in prevention of the diseases in a global measure is one thing, but educating the population who are acting out of false perception and misinformation is another (20). The ultimate advice for cases similar to this specific one is to contact medical professionals who are well informed around the topic and avoid basing their decisions off of hearsay and inaccurate information (20).
Bibliography
Contributors w. MMR vaccine [Internet]. En.wikipedia.org. 2019 [cited 18 October 2019]. Available from: https://en.wikipedia.org/wiki/MMR_vaccine
Pappas S. How Do Vaccines Work? [Internet]. livescience.com. 2010 [cited 18 October 2019]. Available from: https://www.livescience.com/32617-how-do-vaccines-work.html
Sokolova v. The potential of nanoparticles for the immunization against viral infections [Internet]. Royal society of chemistry. 2015 [cited 18 October 2019]. Available from: https://pubs.rsc.org/en/content/articlelanding/2015/tb/c5tb00618j#!divAbstract
Pollard A. Measles | Vaccine Knowledge [Internet]. Vk.ovg.ox.ac.uk. 2019 [cited 18 October 2019]. Available from: http://vk.ovg.ox.ac.uk/vk/measles
Hendriks j. Measles Vaccination Before the Measles-Mumps-Rubella Vaccine. Am J Public Health [Internet]. 2013 [cited 18 October 2019];103(8)(103(8):1393–1401. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4007870/
Deciding not to give my child MMR (measles, mumps and rubella) | Topics, Immunisation, Pregnancy & children, People’s Experiences | healthtalk.org [Internet]. Healthtalk.org. 2019 [cited 18 October 2019]. Available from: http://www.healthtalk.org/peoples-experiences/pregnancy-children/immunisation/deciding-not-give-my-child-mmr-measles-mumps-and-rubella
Gans H. UpToDate [Internet]. Uptodate.com. 2019 [cited 18 October 2019]. Available from: https://www.uptodate.com/contents/measles-epidemiology-and-transmission#H2
Measles outbreaks across England [Internet]. GOV.UK. 2018 [cited 18 October 2019]. Available from: https://www.gov.uk/government/news/measles-outbreaks-across-england
Factsheet about measles [Internet]. European Centre for Disease Prevention and Control. 2019 [cited 18 October 2019]. Available from: https://www.ecdc.europa.eu/en/measles/facts/factsheet
Belluz J. 8 things everybody should know about measles [Internet]. Vox. 2019 [cited 20 October 2019]. Available from: https://www.vox.com/2019/1/29/18201982/measles-outbreak-virus-vaccine-symptoms
Characteristics of Infectious Disease | Microbiology [Internet]. Courses.lumenlearning.com. 2019 [cited 20 October 2019]. Available from: https://courses.lumenlearning.com/microbiology/chapter/characteristics-of-infectious-disease/
New support for measles vaccine to help save more than one million lives [Internet]. gavi.org. 2015 [cited 20 October 2019]. Available from: https://www.gavi.org/library/news/press-releases/2015/new-support-for-measles-vaccine-to-help-save-more-than-one-million-lives/
Understanding thimerosal vaccines and vaccine safety [Internet]. Cdc.gov. 2013 [cited 22 October 2019]. Available from: https://www.cdc.gov/vaccines/hcp/patient-ed/conversations/downloads/vacsafe-thimerosal-color-office.pdf
Thimerosal in Vaccines Thimerosal | Concerns | Vaccine Safety | CDC [Internet]. Cdc.gov. 2015 [cited 22 October 2019]. Available from: https://www.cdc.gov/vaccinesafety/concerns/thimerosal/index.html
vaccines gone viral [Internet]. villavirus. 2019 [cited 22 October 2019]. Available from: http://villavirus.web.unc.edu/tag/ethylmercury/
elliman d. MMR: where are we now? [Internet]. pubmed. 2007 [cited 22 October 2019]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2066086/
chirstie b. Scottish expert group finds no link between MMR and autism. pubmed [Internet]. 2002 [cited 22 October 2019];324(7346)(324(7346). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1172158/
Conducting health communication activities on MMR vaccination [Internet]. Ecdc.europa.eu. 2010 [cited 23 October 2019]. Available from: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/1008_TED_conducting_health_communication_activities_on_MMR_vaccination.pdf
Measles, Mumps, and Rubella (German Measles) – Vaccines – ProCon.org [Internet]. Vaccines. 2017 [cited 23 October 2019]. Available from: https://vaccines.procon.org/vaccine-histories-and-impact/mmr/
Storr C. Measles Status—Barriers to Vaccination and Strategies for Overcoming Them [Internet]. pubmed. 2018 [cited 23 October 2019]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6293121/