Essay on Compare and Contrast 3 Leadership/Management Styles Which Are Relevant to Health/Social Care
Number of words: 2169
Introduction
Leadership is something which has frequently been disseminated in literature and academic circles- particularly its relevance to performance, optimisation of resources (such as allocation/distribution of them) and managing of employees (which can be dependent on their competencies and personality, something which will be elaborated in more depth at a later stage in this composition). The complexity and equivocal nature of leadership is perhaps the reason why it has enthralled and engrossed scholars across the globe- with several researches and studies conducted into it to explore its complexities and whether it is indeed an innate attribute or actually that it is something which can be cultivated, propagated and nurtured.
Leadership in Literature
Leadership styles are frequently scrutinised in literature (with various views and opinions as to which leadership style is feted and should be placed at the pinnacle of the assortment of all the various leadership styles conjugated by various theorists) and the relevance of it to specific industries and disciplines (business, education and psychology are perhaps at the forefront of the mind when conversing of leadership). Even within the early stages of this piece of academic prose, the point that leadership is a complex and multi-faceted field of study is evident. Health and Social Care (like any discipline associated with leadership) is also a complex industry, with the style of leadership demonstrated often dependant on other supplementary factors- i.e. the nature and severity of the patient’s condition, the branch of health and social care which the practitioner is practicing within and the organisational culture which the institution/organisation operates within (Schein, 1992). In Schein’s definition at least, this refers to the attitudes of an organisation, the behaviours inherent in it and the principles which the organisation levies/stands by. Although this is a generic definition, it lends a certain malleable quality to it- in that it can be applied to all disciplines/sectors of work. Due to this transferable nature of the concept, it could be hypothesised that the behaviours which are inherent within an organisation refer predominantly to the leadership style which is on offer in that particular organisation.
Rationale for selecting the 3 styles of leadership
Given the limited wordage of this assignment (and due to the requirements of the essay brief), only 3 leadership styles can be ‘compared and contrasted’ (critically appraised to see whether they are similar or disparate in nature). Due to a mixture of their relevance to Health/Social care (Gopee and Galloway, 2009, 2014) and their good standing in the literature, situational, transformational and democratic styles of leadership are included in this assignment. These, along with autocratic leadership, are perhaps the most well-known and reputable in public knowledge and in literature. Autocratic (also known as authoritarian) leadership was devised by Lewin et al. (1939) and mainly entails a leader having direct control over their followers/sub-ordinates, dictating to them their roles and duties, with not even a mere scintilla of collaboration in presence. As partial justification for its exclusion from this assignment, Autocratic leadership has often been associated with a reign of tyranny and oppression, where followers have no choice other than to comply with their leader (or in more pejorative parlance, dictator) or else face dire consequences (which in an employment context could be instant dismissal or sanctions) (Bass and Bass, 2008). As well as the theory being out-dated and possibly irrelevant to the contemporary era (as mentioned previously, it was conceptualised in 1939), it may be anathema to good working practices with Bass and Bass (2008) describing it in unflattering terms as being ‘punitive, close-minded and coercive’. Thus, the selection of the three leadership styles seems to be a sound and informed decision.
Leadership in Health/Social Care and Comparison of the three leadership styles
Prior to entering a comparison of the three leadership styles (which encompasses a definition, theoretical evaluation and consults healthcare perspectives on the matter), it seems pertinent to clarify succinctly why leadership is so important in health and social care. In consulting authoritative, subject-specific literature, this becomes clear. Jones and Bennett (2012), in their authoritative tome which aims to assist emerging leaders in healthcare make the point that leadership is evident in all levels of an organisation, philosophising that whichever role or position one holds in an organisation, they can make a difference. However, they definitively state that if one displays leadership qualities in their role, then their contribution can be magnified still further.
Even without consulting literature, to an external observer the need for leadership in any health and social care setting is seemingly irrefutable, due to the diverse nature of the profession. With the infinite amount of different duties, responsibilities and disciplines which are existent in the area of healthcare, there could be a potential danger of employees or personnel adopting roles which are not part of their remit, thus possibly resulting in less than exemplary practice. Arguably, a leader is needed to ensure that the practice of an organisation is cohesive and runs smoothly, with no disruptions or aberrations being made. Martin et al. (2010) collaborates this notion: promulgating that in the many contexts which a manager must work within (multi-agency and multi-disciplinary work), sound leadership is of paramount importance. This is because leadership is needed to co-ordinate each professional and ensure that they are fulfilling their duties correctly. In this sense, the assumption could be made that the leader must be skilled and adept at working in many different contexts. This refers to the modality of situational leadership, where a leader has the ability to tailor their leadership skills to the situation (or scenario/context) that they find themselves implicated within (Bass and Bass, 2009). The original theorists who conceptualised situational leadership were Hersey and Blanchard (1977), although this has been refined and amended by subsequent theorists (i.e. Bass and Bass, 2009). Hersey and Blanchard (1977) thought that there were 4 styles of leadership, which were dependent on the capability and willingness of the employees:
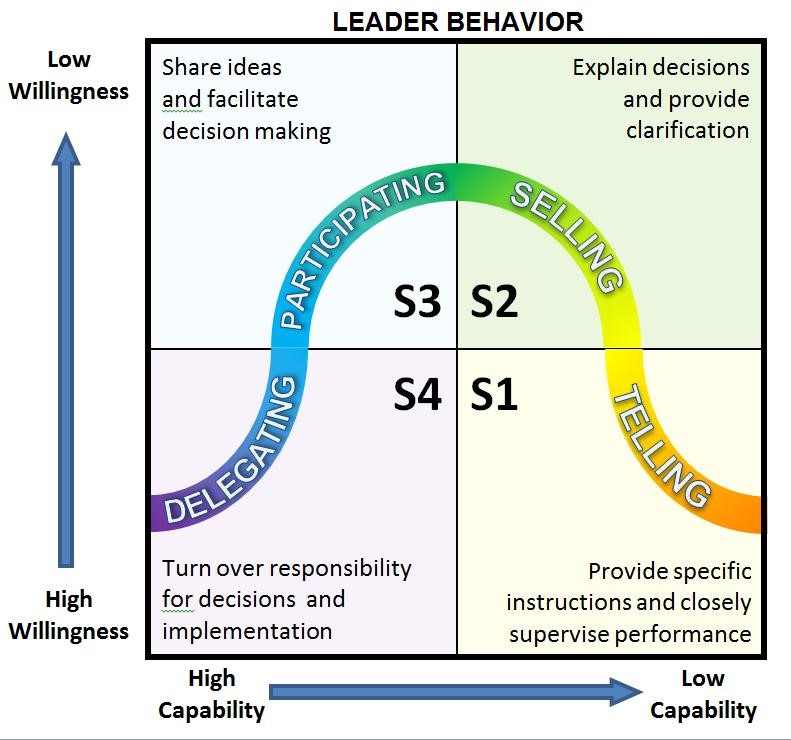
Figure 1- Matrix of Hersey and Blanchard’s (1977) Situational Leadership Model
This style of leadership is also given some backing by the literature. Brown et al. (2010) argue that the style of leadership which is espoused by the leader will inevitably depend on the situation they are in a health/social care context, as well as the ‘different developmental levels’ of the staff under their jurisdiction. This strand of reasoning arguably bares some similarities to Hersey and Blanchard’s (1977) model in enunciating that leadership is reliant on the qualities of the staff who are under the direction of the leader. However, this notion is not uniformly praised in literature pertaining to health/social care. Taking an alternative perspective on matters, Gopee and Galloway (2014) are advocates/proponents of the transformational leadership style. Defining this, Bass and Riggio (2006) note that transformational leaders are capable of stirring great change, even in organisations where morale is low and employees’ spirits may have been dampened for some reason (subjectively, in the Health and Social Care setting this could be due to insufficient working conditions and financial recompense). The inference is made here that transformational leaders are inspiring figures who do not command respect (as would be more typical of an autocratic/dictatorial regime), instead earning it through respecting their employees’ opinions and encouraging them to ‘buy into’ (Bass and Bass, 2008) the ethos which they espouse. However, this viewpoint almost seems to glamorise the assets and efficacy of transformational leadership, with it potentially only being applicable to health and social care settings where employees need inspiring (with the assumption made that health and social care employees are predominantly motivated intrinsically or through altruistic, empathetic principles rather than financial means/resources). Arguably, in such environments, a democratic (or egalitarian) model of leadership needs to be demonstrated, which is where employees’ needs are respected, their concerns are dealt with and taken into account and also where ‘leaders’ and followers are on a more even footing (Woods, 2010). This seems to exhibit some similarities with the transformational leadership style, as both have a collaborative component to them, although this is visible in different ways. In the transformational leadership model, the leader is seen to be the visionary, showing a penchant (or proclivity) for inspiring others and encouraging (not forcing) them to follow them. Contrastingly, in the democratic leadership model, the emphasis is more on leaders and followers collaborating together to construct a shared vision, rather than the leader solely devising one and influencing employees to follow their line of reasoning. Such a close interaction between transformational and democratic modalities of leadership seems to place situational leadership (which depends more on the context that one is operating within rather than the ethos/personality of the leader) in a different dimension to the previously mentioned styles of leadership. Nevertheless, there is arguably still some connection between the leadership styles. The first is that they involve the leader to demonstrate more than a mere semblance of interpersonal/psychological intelligence: democratic (in considering employees’ needs), transformational (using techniques to influence employees and persuade them to join the leader’s vision) and situational (understanding both employees’ level of enthusiasm and competency and demonstrating the corresponding leadership style to display to them). This association between the leadership styles is reaffirmed by literature with Goleman (1996) advising that emotional (interpersonal) intelligence is better a predictor of success in life and employment than academic aptitude and acumen.
Perhaps the biggest differentiator between when the leadership styles are employed is the level leadership needs to be displayed at and the volume of people who are commanded by it. The assumption that leadership is only demonstrated at the upper echelons of the organisation in managing the employees that are beneath them may be invalid, as arguably leadership is demonstrated at all levels in any organisation. For instance, transformational leadership may be required to sway a vast amount of people (particularly in a flagging workplace), situational leadership might only be needed with a group or set of individuals, whereas democratic leadership may arguably be demonstrated by those whom are situated at a lower point in the hierarchy of an organisation than more ‘stereotypical’ leaders. In a health setting, this may be nurses displaying clinical reasoning in directing the patients who are under their care and considering their needs (which is synonymous with a patient-centred care model) (Higgs, 2008). Or in a social care setting, this may be to organise group work for various individuals and will involve consideration of the individual’s needs (e.g. cognition, mobility and responsiveness) and ensure that they are adequately catered for (Preston-Shoot, 2007).
Conclusion
Fundamentally, all three leadership styles are similar in that they require a leader to demonstrate interpersonal intelligence, but differ according to the situation/context that they need to be demonstrated in. Arguably, amongst the three identified in the context of this assignment at least, there is no superior leadership style. Rather, a leader should have the capacity to demonstrate all three, potentially concomitant to each other, particularly in the volatile health and social care industry.
References
Bass, B. and Riggio, E. R. (2006) Transformational Leadership. New York: Psychology Press.
Bass, B. M. and Bass, R. (2008) The Bass Handbook of Leadership: Theory, Research, and Managerial Applications. New York: Free Press.
Bass, M. B. and Bass, R. (2009) The Bass handbook of leadership: Theory, Research and Managerial applications. New York: Simon and Schuster.
Brown, K. [et al.] (2010) Effective Leadership, Management and Supervision in Health and Social Care. London: Sage.
Cook, M. J. (2001) ‘The Renaissance of clinical leadership’, Int Nurs Rev, 48 (1): 38-46.
Goleman, D. (1996) Emotional Intelligence: Why it can matter more than IQ. New York: Bloomsbury Publishing.
Gopee, N. and Galloway, J. (2009) Leadership and management in Healthcare. London: Sage.
Gopee, N. and Galloway, J. (2014) Leadership and management in Healthcare. 2nd edn. London: Sage.
Jones, C. and Bennett, C. L. (2012) Leadership in Health and Social Care: An introduction for Emerging Leaders. London: Royal College of General Practitioners.
Hersey, P. and Blanchard, K. H. (1977) Management of Organizational Behavior 3rd Edition– Utilizing Human Resources. New Jersey/Prentice Hall.
Higgs, J. (2008) Clinical reasoning in the Health professions. Boston: Elsevier Health Services.
Lewin, K. [et al.] (1939) ‘Patterns of aggressive behavior in experimentally created social climates.’ Journal of Social Psychology, 10, 271-301.
Martin, V. [et al.] (2010) Managing in Health and Social Care. London: Routledge.
Schein, E. (1992) Organizational Culture and Leadership: A Dynamic View. San Francisco, CA: Jossey-Bass.
Preston- Shoot, M. (2007) Effective Group Work. Basingstoke: Palgrave.
Woods, A.P. (2010) ‘Democratic leadership: drawing distinctions with distributed leadership’. International Journal of Leadership in Education, 7 (1): 3–36.